
Stethoscope acoustics
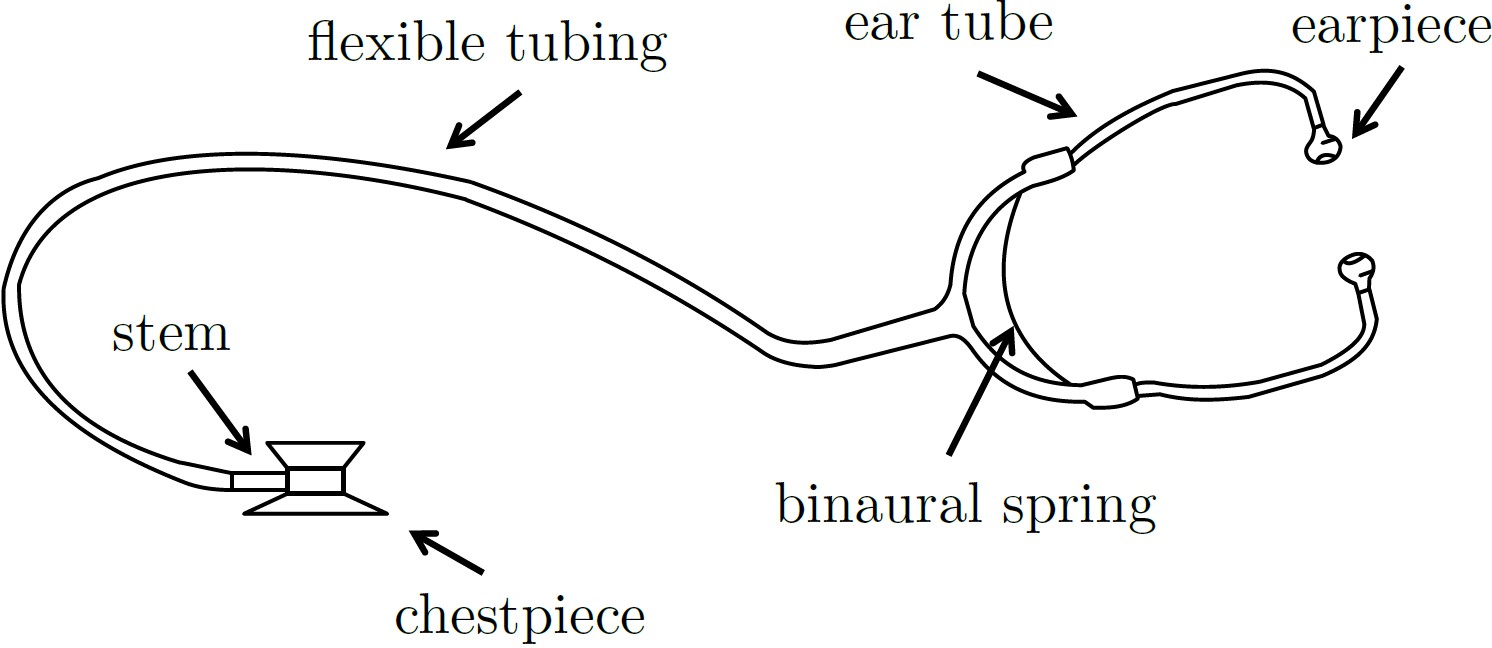
The stethoscope was invented over 200 years ago and has become a symbol of the medical profession. A typical ‘traditional’ stethoscope now consists of a chestpiece, flexible tubing and earpieces. The acoustics properties of stethoscopes are surprisingly complex. This has led to a number of misconceptions about how stethoscopes work throughout the academic and medical literature, as well as in lay explanations of stethoscope acoustics.
We have developed a theoretical acoustic model for understanding the behaviour of stethoscopes. In order to inform and validate our theoretical work, we have developed a range of experimental techniques. These include careful processing of data collected on human chests to account for natural variability, as well as the use of laboratory “phantoms”. In this context a “phantom” is a test-setup that mimics the behaviour of the human chest and allows detailed and repeatable experiments to be conducted.
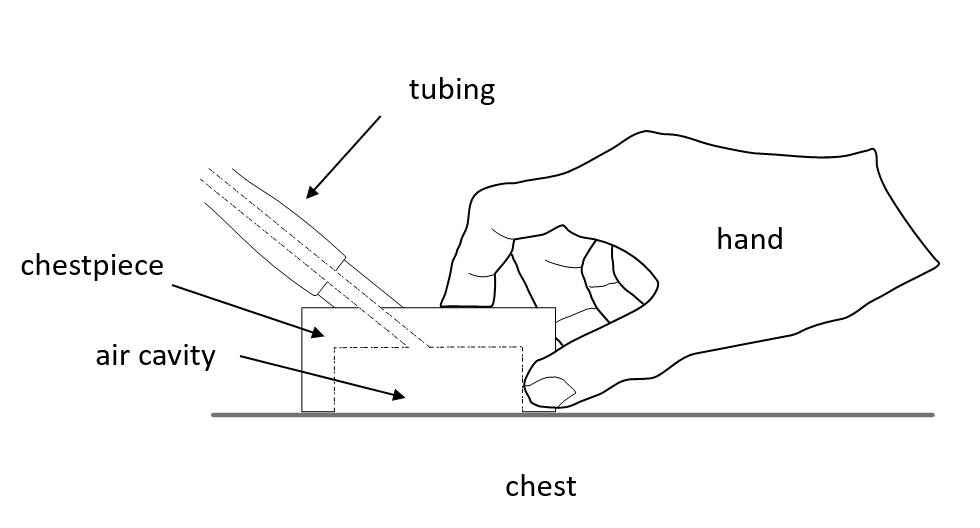
The complexity of stethoscope acoustics stems from the fact that stethoscopes interact with human tissue in three ways: at the chest of the patient, at the hand of the clinician and at the ear of the clinician. Each of these interactions plays a key role in determining the transmission of vibrations from the body of the patient to the ear of the clinician. When a clinician presses a stethoscope chestpiece against the chest of the patient, a coupled system is formed. The mechanical properties of this coupled system depend not only on the properties of the stethoscope itself, but also on the properties of the chest and the way in which the stethoscope is held.
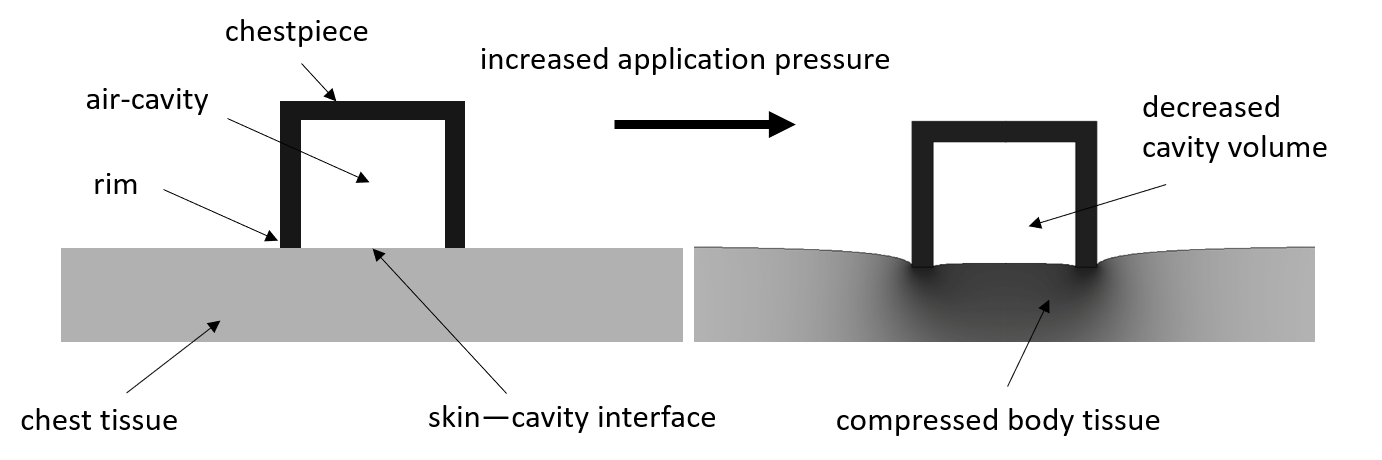
Many widely quoted statements about stethoscope performance are based on experiments that do not accurately account for the coupling of the stethoscope to the chest leading to misleading recommendations. Our work aims to dispel these misconceptions and provide a clear framework for understanding and modelling the physics of stethoscopes.
